
Groin injuries, encompassing adductor strains, tendinopathies, and hip-related pain, affect up to 28% of male soccer players annually and sideline athletes across sports like running, tennis, and field hockey. The Copenhagen adduction exercise (CAE)—often performed as a side plank variation—has emerged as a cornerstone intervention due to its high neuromuscular demand on the hip adductors.
Adductors: The Forgotten Stabilizers
Adductors are the forgotten workhorses of lower body training—overlooked while quads, hamstrings, and glutes steal the spotlight in squats, deadlifts, and lunges. Most programs ignore these inner thigh muscles until a groin tweak sidelines you mid-sprint or cut, revealing their critical role in pelvic stability, explosive direction changes, and injury prevention. Unlike flashier moves, adductor isolation demands intention: without targeted work like Copenhagen planks, they weaken relative to antagonists, spiking strain risk by 4x in sports demanding eccentric control.
Epidemiology and Risk Factors for Groin Injuries
Groin problems account for 12-18% of all sports injuries, with adductor longus strains being most common. Risk factors include previous injury (odds ratio 2.8-6.6), age over 25, and eccentric hip adduction weakness relative to abduction.
Biomechanics and Neuromuscular Effects
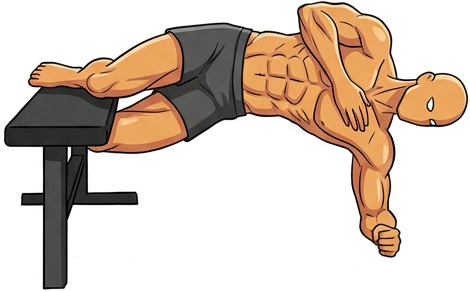
CAE involves side-lying isometric hip adduction against a bench or partner’s shoulder, emphasizing eccentric control as the top leg lowers. Electromyography (EMG) studies reveal superior activation: adductor longus reaches 108% of maximum voluntary isometric contraction (MVIC)—higher than ball squeezes (49%) or slide variations.
A 2021 systematic review of five studies found CAE significantly boosts eccentric hip adduction strength (EHAD) in all four trials assessing it, eccentric hip abduction (EHAB), and EHAD:EHAB ratio in three of three. It also elevates adductor EMG by 108% in the dominant leg, providing a potent strengthening stimulus.
Mechanistically, CAE trains the adductors’ role in pelvic stability during single-leg stance, countering the lengthening contractions in sports like sprinting or changing direction.
Evidence for Rehabilitation
In rehab, CAE shines. A 2024 on soccer players with adductor-related groin pain showed a CAE-inclusive program improved EHAD strength, hip ROM, self-reported disability, and pain more than standard rehab. Post-8 weeks, intervention groups had superior outcomes.
Holmich et al.’s protocol integrates CAE for return-to-play, with strong evidence for adductor strengthening reducing reinjury. Clinically relevant pain reductions occur even in non-significant trials, tied to compliance.
Evidence for Prevention: Promising but Mixed
Prevention data is nuanced. A 2025 review found small, non-significant groin injury risk reduction across three trials, with one showing. High-compliance programs cut seasonal prevalence from 21.3% to 13.5%.
Harøy et al. reported 31% adductor strain drops preseason. However, Grade B evidence questions standalone CAE for prevention, favoring multimodal programs. Benefits include no equipment needs and performance perks like improved balance.
Beginner Technique and Cues
Ideal for home gyms: Use a bench, box, or bed edge.
- Lie on your side.
- Beginner (knee variation): Top knee on support; bottom leg hooked underneath.
- Lift hips to align shoulders-knees-feet; squeeze adductors.
- Hold 10-30s; 3-4 sets/side.
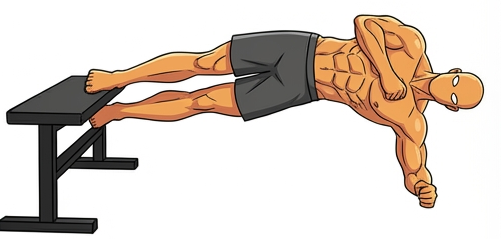
Advanced Variations and Progressions
- Foot/ankle variation: Top ankle on support for longer lever arm (+20-30% EMG).
- Pulses: 2s eccentric lowers at peak hold.
- Dynamic: Slow lowers (3-5s) for eccentric overload.
Conclusion: Essential Tool for Adductor Resilience
CAE’s high activation, rehab efficacy, and accessibility make it indispensable for groin health. Consistent use yields measurable strength gains and pain relief, aligning with your evidence-based home programming. Implement today—your athletes will stay on the field longer.
